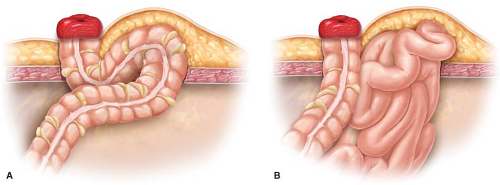
A hernia is an abnormal growth of the bowel at the abdominal wall. It occurs on a weak part of the walls. It mainly affects the stomach or the intestines. A large protrusion often forms around and the intestines. The size of this protrusion depends on the size of the area, which was weak, and the stoma came through. If the size of the weakened area is small, then a small protrusion forms, but if the size of the weakened area is big, then a big protrusion that is noticeable will form. A hernia around the stoma is what we refer to as parastomal hernias.
This condition affects 5% to 10% of people with colostomies and 3% to 10% of people with ileostomies. It is difficult to tell who can get parastomal hernias and who can't. However, some factors make people vulnerable to contracting this complication. They include;
Site of the stoma
When a stoma is made outside the rectus abdominus muscle, then you can get a hernia around the stoma.
Age
The older you become, the weaker your muscles become. When this affects the abdominal muscle, then herniation can happen at any given time.
Obesity
People with excess weight are more vulnerable to getting a hernia because their weight puts too much pressure on abdominal muscles, making them weaker hence the possibility of a hernia.
Malnutrition
Poor eating habits especially lack of a balanced diet during the stoma surgery recovery period, is dangerous. This is because it might delay the normal healing of the abdominal wall, which is a sign of weakness.
Infection after stoma surgery
An infection might eat up muscles and eventually create a weakness on the abdominal walls.
Increased intra-abdominal pressure
This pressure exerted on the abdominal muscles might come from frequent severe sneezing, lifting of heavyweights, and chronic coughing. This pressure, especially from the heavyweights, is dangerous because it can even cause muscles to tear.
Parastomal hernias may develop very soon after surgery or may take years to build these depending on the patient's condition. 80 % of people who have undergone surgery do not struggle with a hernia. People with a hernia learn how to deal with it after medical intervention.
People often describe Parastomal hernia through its abdominal discomfort. It causes a feeling of fullness in the parastomal area that is not painful but is however uncomfortable. This is dealt with by supporting the hernia with a unique elastic hernia belt. A lycra-type undergarment can also help to make you comfortable. Belts need to be measured accurately to fit your abdomen. If you are having severe pain resulting from the stoma or hernia, you should seek help from an Enterostomal Therapy nurse. The nurse helps you to choose between a belt and a lycra undergarment.
According to your movements, a parastomal hernia can also change the size and shape of the stoma. This may cause a leak in your appliances and even lead to skin problems. When you cannot see your stoma to take care of it, you should contact your nurse for assistance. The hernia affects the normal functioning of the stoma.
In conclusion, the parastomal hernia can be avoided, and in case you get it, it can be dealt with well with the help of medical professionals.







